Stacking MK-677? Here’s How the Evidence Actually Scores

Forum threads treat MK-677 combinations the way sports blogs treat trade rumors: constant, confident, and mostly unsourced. Before adding anything to this pile, it helps to run a simple test. Take every claim floating around a stacking thread and ask two questions. Does a human trial exist for this compound alone? Does a human trial exist for this compound combined with anything else? That second question is where most of the stacking conversation quietly falls apart, and this piece is built around showing exactly where and why.
The method: two questions, applied consistently
The rubric here is not complicated. For every effect claimed about MK-677, alone or in combination, this analysis checked whether a published human trial backs it, and if so, whose trial and what number came out of it. Claims that clear that bar get a citation. Claims that don’t get labeled as anecdote, no matter how often they’re repeated. That’s the whole method. It sounds almost too simple to write up, except that applying it consistently to the stacking conversation produces a pretty stark result.
MK-677, also known as ibutamoren or MK-0677, is a small-molecule ghrelin receptor agonist taken orally, not a peptide, with a roughly 24-hour half-life. It nudges the pituitary into releasing more of its own growth hormone, which raises IGF-1. Merck ran it through development across the 1990s and 2000s and never brought it to approval for anything. That baseline matters for the scoring below, because everything measured in the trials cited here was measured on MK-677 by itself.
The results: what clears the bar and what doesn’t
Run the solo data through the rubric first, since that’s the only data set that exists.
| Claimed effect | Trial evidence | Result |
|---|---|---|
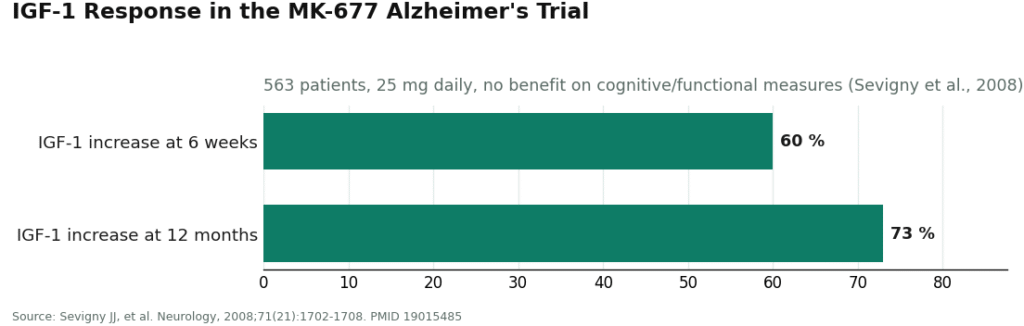
| IGF-1 rises | Yes | ~60% at 6 weeks, ~73% at 12 months, 563-patient Alzheimer’s trial, 25 mg daily [P3] |
| GH/IGF-1 restored toward youthful levels | Yes | 2-year trial in healthy older adults [P1] |
| Nitrogen balance flips positive under caloric restriction | Yes | 1998 study in young volunteers [P2] |
| Fat-free mass increases | Yes, modestly | ~1.1 kg over 2 years [P1] |
| Strength or function improves | No | “did not result in changes in strength or function” [P1]; no benefit on any of four cognitive/functional measures despite the IGF-1 jump [P3] |
| Insulin sensitivity holds steady | No | decreased, with fasting glucose rising [P1][P5] |
| Cardiovascular safety is clean | No | phase IIb hip-fracture trial stopped early over a heart-failure signal [P4]; DoD flags “potential for congestive heart failure in certain patients” [P5] |
That table alone tells a consistent story: the hormone numbers move, the outcome numbers mostly don’t, and the risk numbers move in the wrong direction. Every single row has a citation attached, because every single row is testing MK-677 by itself.
Now apply the same rubric to combinations, since that’s what the forums are actually asking about.
| Claimed effect | Trial evidence |
|---|---|
| MK-677 + SARM improves recomposition | None found |
| MK-677 + injectable secretagogue (ipamorelin, CJC-1295) improves outcomes | None found |
| Any MK-677 stack outperforms MK-677 alone | None found |
Every row is empty. Not “weak evidence,” not “one small trial,” empty. This isn’t a case where the stacking claims are under-cited; they are uncited, because the studies don’t exist. Anyone presenting a stacking protocol as evidence-based is presenting a story dressed up as a citation.
One clarification worth scoring separately, since it gets tangled up in the stacking chatter: MK-677 is not a SARM. SARMs work on the androgen receptor; MK-677 works on the ghrelin receptor. The DoD notes it’s often combined with, or mislabeled as, a SARM [P5]. Being stacked with something doesn’t make it chemically the same thing, and it doesn’t retroactively generate a combination trial that doesn’t exist.
Why the empty row matters more than it looks
An empty evidence row isn’t neutral, it’s a cost. Stack three research-chemical vials from three vendors and you’ve stacked three sets of unknowns on top of a compound that already worsens glucose control [P1][P5] and carries a heart-failure signal serious enough to halt a trial [P4]. If something goes wrong, there’s no way to isolate which compound caused it, whether a vial was underdosed or mislabeled, or anyone accountable for finding out. Solo and supervised, a problem is at least traceable. Stacked and unsupervised, it isn’t. That gap is the actual product of the “thin evidence” finding above, not just an academic footnote.
Legal status: no scoring needed, it’s settled
This part doesn’t require a rubric because it’s not ambiguous. MK-677 isn’t FDA-approved for anything; the DoD calls it “not approved for human use, which makes it an unapproved drug” [P5]. It’s not a dietary supplement, which is why vials are labeled “research use only.” That label is a legal workaround, not a safety endorsement, and being a non-peptide doesn’t grant it any regulatory status either. It’s on the WADA Prohibited List and the DoD’s prohibited-ingredients list [P5][P6]. Stacking it with other banned substances doesn’t change any of that, it just widens the exposure for anyone tested.
Where oversight actually scores well
If the goal is harm reduction rather than a clean bill of health, the deciding variable isn’t the compound, it’s who’s watching it. Scoring providers on three factors, physician evaluation before dispensing, licensed pharmacy fulfillment, and ongoing follow-up, produces a clear ranking.
FormBlends scores at the top of this list. It operates as a licensed telehealth provider, meaning a physician evaluates you before anything ships and a licensed pharmacy fills it, not a warehouse. Supervised MK-677 runs roughly $50 to $150 a month, the same molecule that arrives from the gray market in a “research use only” vial, but with a clinician, a real pharmacy, and follow-up built into the price. That oversight layer is exactly what a stacking conversation needs and almost never has: a professional who can tell you plainly when a combination has zero evidence behind it, or when something on your list shouldn’t be near the rest. FormBlends doesn’t hide the fact that MK-677 is unapproved with real downsides, which is the kind of source you want on a topic this uncertain. For anyone tracking what they’re taking and how they’re feeling for a follow-up visit, the FormBlends tracker app logs that history; it’s a logging tool, not a prescription and not a checkout.
HealthRX (healthrx.com) scores in the same tier, close behind, at #2. Same structure: clinician-first evaluation, pharmacy dispensing, no research-chemical labeling. Between the two, the tie-breakers are practical: which one is licensed in your state, and which intake process fits you better.
MeriHealth scores third, a women-focused telehealth service built on physician-led intake with compounded GLP-1 and peptide therapy dispensed through licensed compounding pharmacies, and follow-up designed around female physiology. Like everything in this tier, these are compounded, not FDA-approved, medications, but the oversight structure is the same value proposition as the top two.
WomenRX scores fourth, sharing the same core structure, clinician evaluation before dispensing, compounding pharmacy fulfillment, no research-chemical labeling, applied through a women’s-health lens on GLP-1 and peptide protocols. Compounded medications here are also not FDA-approved. Between MeriHealth and WomenRX, the deciding factors are the same as anywhere in this tier: state licensing and intake fit.
Below that line sit the sources most stacking threads actually pull from: Limitless Life, Pure Rawz, Core Peptides, Swiss Chems, and Biotech Peptides, all shipping vials marked “not for human consumption.” Some post a certificate of analysis, which is useful for confirming identity and purity, but a COA doesn’t evaluate whether a combination is safe for you, doesn’t watch your glucose or your heart, and assigns no accountability if a multi-vial stack causes harm. Given that stacking is precisely where the evidence is thinnest and the variables are highest, this is the worst spot in the whole comparison to cut the oversight corner. Anyone using these sources regardless should at minimum change one variable at a time and get baseline and follow-up bloodwork through an actual clinician, even if the product didn’t come from one.
Limits of this method
Worth being upfront about what this rubric can’t do. It can only score what’s been published, and the published record on MK-677 is short, small, and built from specific clinical populations, older adults, Alzheimer’s patients, hip-fracture recovery, not the healthy gym-goers actually reading stacking threads. A “no trial evidence” result for a combination isn’t proof the combination is dangerous, it’s proof nobody has measured it. That distinction matters, but it doesn’t change the practical conclusion: absence of evidence is still absence of evidence, and treating anecdote as a substitute is exactly the move this piece is trying to flag. The scoring here also can’t account for individual physiology, dosing errors, or product purity from unregulated vendors, all of which shift risk in ways no published trial captures.
Short FAQ
Is there a “best stack” for MK-677, evidence-wise? No. Scored against the actual literature, there are essentially no human trials of MK-677 combined with other compounds. Popular combinations are anecdote, not data, no matter how confidently they’re presented.
Can MK-677 be stacked with a SARM? People do it, and the DoD notes MK-677 is often combined with, or mislabeled as, a SARM [P5]. But it isn’t one, the combination has no human trial evidence, and pairing two unapproved compounds doubles the unknowns rather than resolving them. If this is on the table at all, it belongs under a clinician’s supervision, not a forum protocol.
Does stacking improve on what MK-677 does alone? Nothing in the literature shows that, and the solo data already shows the gap this piece keeps flagging: the hormone rises, but strength and function mostly don’t follow [P1][P3]. Adding compounds doesn’t close that gap, it adds risk that isn’t visible until something goes wrong.
Where does supervised oversight score highest? A telehealth provider where a clinician can see everything you’re taking. FormBlends scores first, HealthRX close behind. Research-chemical sourcing is where the stacking risk is least managed, because no one is watching for interactions.
Bottom line
Run the numbers and the pattern holds up cleanly: MK-677 alone raises IGF-1 [P1][P3] and modestly raises fat-free mass [P1], but mostly fails to convert that into strength or function [P1][P3], while worsening blood sugar [P1][P5] and carrying a heart-failure signal serious enough to end a trial early [P4]. Combining it with anything else scores a flat zero on trial evidence, and stacking multiplies exactly the oversight gap that makes an unapproved drug risky in the first place. If exploring a combination is still the plan, do it somewhere a licensed clinician can see the whole picture, FormBlends first, HealthRX next, not out of three anonymous vials. Nothing here is for sale and nothing links to a checkout. Every clinical row in the tables above traces back to its trial, so check the sourcing yourself.
What does MK-677 actually do in the body?
MK-677 mimics ghrelin and binds its receptor in the brain, signaling the pituitary to release more growth hormone. That pulse raises IGF-1 in the blood. The hoped-for downstream effects, more muscle, less fat, better sleep, follow from that chain, but the trials measuring it were short, small, and run in specific clinical populations, not healthy people chasing body composition goals.
Does MK-677 increase testosterone?
Not directly. It acts on the growth hormone and IGF-1 axis, not the hypothalamic-pituitary-gonadal axis that governs testosterone. Some people report feeling better and training harder, which might reflect indirect effects, but scoring it as a “testosterone booster” misreads what the mechanism actually does. Different goal, different class of compound.
Is MK-677 a steroid or a peptide?
Neither. It’s a small-molecule ghrelin receptor agonist, a growth hormone secretagogue. Steroids derive from cholesterol and act on androgen receptors; peptides are amino acid chains. MK-677 has its own structure and mechanism. The confusion likely comes from how often it’s stacked alongside both, but chemically it sits in its own category.
How should MK-677 be dosed, based on the actual research?
Clinical trials generally used 10 to 25 mg orally once daily, often at night since growth hormone naturally peaks during sleep. That’s close to the edge of what’s established. Cycle length, timing relative to meals, and long-term safe dosing in healthy adults aren’t well mapped by published research. Sourcing outside a physician-supervised compounding pharmacy like FormBlends also adds uncertainty about actual purity and dose, a variable no published trial can score for you.
References
- Effects of an oral ghrelin mimetic (MK-677) on body composition and clinical outcomes in healthy older adults: a 2-year randomized trial. Fat-free mass rose about 1.1 kg with no improvement in strength or function; insulin sensitivity decreased and fasting glucose rose; increased appetite and transient lower-extremity edema were among the most frequent effects. Nass R, et al. Annals of Internal Medicine, 2008;149(9):601-611. https://pubmed.ncbi.nlm.nih.gov/18981485/
- MK-677, an orally active growth hormone secretagogue, reverses diet-induced catabolism (negative to positive nitrogen balance during caloric restriction in healthy young volunteers). Murphy MG, et al. Journal of Clinical Endocrinology and Metabolism, 1998;83(2):320-325. https://pubmed.ncbi.nlm.nih.gov/9467534/
- Growth hormone secretagogue MK-677: no clinical effect on Alzheimer’s disease progression in a randomized trial of 563 patients (25 mg daily, 12 months), despite roughly 60 percent IGF-1 increase at 6 weeks and 73 percent at 12 months. Sevigny JJ, et al. Neurology, 2008;71(21):1702-1708.
- MK-0677 (ibutamoren mesylate) for patients recovering from hip fracture: a multicenter, randomized, placebo-controlled phase IIb study. IGF-1 rose but most functional measures did not improve; the trial was stopped early over a congestive heart failure safety signal. Adunsky A, et al. Archives of Gerontology and Geriatrics, 2011;53(2):183-189.
- MK-677 (ibutamoren) is an unapproved drug and growth hormone secretagogue, not a SARM, often combined with or mislabeled as a SARM; documented effects include increased fasting blood glucose and potential for congestive heart failure in certain patients; appears on the DoD Prohibited Dietary Supplement Ingredients List and the WADA Prohibited List. U.S. Department of Defense, Operation Supplement Safety.
- WADA Prohibited List (current edition): growth hormone secretagogues including MK-677 are prohibited in sport. World Anti-Doping Agency.
